Current affairs 18th April 2019
Current Affairs and Editorial discussion from various national daily newspapers
Current affairs 18th April 2019
Oumuamua
LAST YEAR, the interstellar object ‘Oumuamua generated worldwide interest — discovered in late 2017, it was then the first known object from outside the Solar System to do a fly-by of Earth.
Now, Loeb and a colleague, Amir Siraj, have proposed that before ‘Oumuamua, there may have been another recent interstellar visitor — a meteor from another solar system may have actually hit Earth in 2014. It burned up in the atmosphere and fell into the South Pacific.
Right to travel
The right to travel abroad is a genuine and basic human right like marriage and family, the Supreme Court has observed in a recent order. “The right to travel abroad is an important basic human right for it nourishes independent and self-determining creative character of the individual, not only by extending his freedoms of action, but also by extending the scope of his experience.
Setting aside the order, the Supreme Court referred to its Maneka Gandhi judgment upholding the right to travel and the U.S. Supreme Court case of 1958 in Kent versus Dulles. The Bench quoted the majority opinion of Justice William O. Douglas in the latter case which said “freedom to go abroad has much social value and represents the basic human right of great significance.
Rise and fall of airlines in India
Evolution of airline industry in independent India
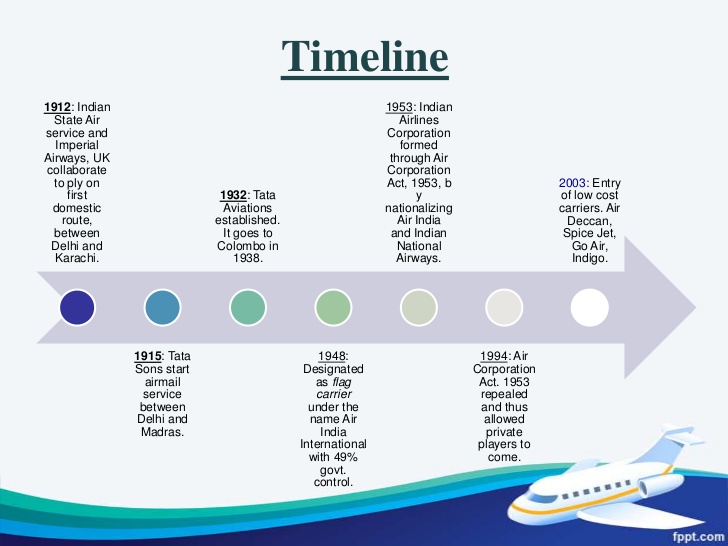
For four decades after eight independent domestic airlines — Deccan Airways, Airways India, Bharat Airways, Himalayan Aviation, Kalinga Air Lines, Indian National Airways, Air India (formerly Tata Airlines), and Air Services of India — were merged to create state-owned Indian Airlines in 1953, India’s aviation sector remained a national monopoly. Policy changes came in the 1990s — and liberalisation and economic reforms gave the private aviation industry new wings of hope.
Several of the private airlines that took off during that decade were to hit air pockets soon, however — and in the years that followed, the sector saw the entry of quite a few new players even as the businesses of others collapsed or were taken over. The suspension of operations at Jet Airways — at one time India’s largest private airline — announced on April 17th 2019, follows the troubles at Kingfisher, Air Deccan, and Sahara.
Liberalisation of air space
Besides repealing The Air Corporation Act 1953, the government announced an Open Skies policy in 1992, liberalising rules and regulations to open up the commercial aviation market. This led to the birth, over the next decade or so, of private sector players including ModiLuft, Damania Airways, Air Sahara, and East-West Airlines. Most of these new players, however, folded up soon or were merged — Jet Airways in contrast, stood out as an efficient private sector operator, gaining market share with each passing year.
In December 2004, the government announced a major policy change, allowing Indian scheduled carriers with a minimum five years’ continuous operations and a minimum of 20 aircraft (the so called 5/20 rule) to fly international routes. Jet was the key beneficiary of this policy change. In 2016, the government scrapped the 5/20 rule and replaced it with 0/20, enabling SpiceJet, IndiGo and GoAir to launch international flights in the following years.
Current trend
Over the last four years, India’s aviation market has grown at a yearly average rate of 20%, among the fastest in the world. More and more Indians are flying; paradoxically though, nearly all the major players are in dire straits financially.
Apart from operational and managerial efficiencies, one of the key determinants of an airline’s success or failure is the price of crude oil. Fuel costs account for roughly 40 per cent of a carrier’s operating cost. Steep taxes on aviation turbine fuel (ATF) in India — one of the highest in the world — make Indian carriers less competitive against global players.

Health reforms in India
Why required?
In the past five years, the Union health budget has stagnated in real terms, allocations to the National Health Mission do not cover inflation and there have been avoidable deaths of scores of children in public hospitals in Gorakhpur and other places that can be ascribed to the lack of material and human resources.
Governments have failed to regulate private hospitals effectively, leading to numerous instances of mismanagement and massive over-charging of patients, such as the tragic case of Adya Singh in Fortis hospital, Gurgaon. There are convincing facts which show that the “solution” being offered in the form of the Pradhan Mantri Jan Aarogya Yojna is not only seriously underfunded (current funds being less than one-fourth of required) but it will only scratch the tip of the iceberg of healthcare requirements in India.
Reforms that may be undertaken
Reforms suggest by Jan Swasthya Abhiyan — a national coalition of health sector organisations and activists -
One, adopting a Right to Healthcare legislation at the Centre and state levels. This would ensure that all residents of the country are entitled to healthcare facilities. Development of a system for Universal Healthcare (UHC) would be a key constituent of this initiative, which would require expansion and strengthening of public health services at all levels. Private providers would also be involved, as per need, to supplement the public health system.
Two, increasing the public health expenditure exponentially through taxation. This expenditure should be increased from the current grossly inadequate 1.2 per cent of the GDP to reach 3.5 per cent of the GDP in the next five years, and eventually touch 5 per cent of the GDP in the medium term.
Three, ensuring major reform and strengthening of public health services with increased staff and infrastructure. A key component of this reform would be guaranteed provision of free essential medicines and diagnostics to all patients in public health facilities, by adopting systems for procurement and distribution which are similar to the current models in Tamil Nadu, Kerala and Rajasthan.
Four, there should be a comprehensive health sector human resource policy, which provides upgraded skill training, fair wages, social security and decent working conditions for all public health services staff. The services of all contractual health workers, including ASHAs and anganwadi workers, should be regularised.
Five, community-based monitoring and planning of health services that are being practised in a few states should be upscaled and user-friendly grievance redressal systems put in place to ensure social accountability and participation.
Six, the PMJAY component of Ayushman Bharat, which is based on a discredited insurance model, should be jettisoned. Such schemes need to be replaced by the universal healthcare system.
Seven, private hospitals must be brought under the ambit of regulations by modifying and adopting the Clinical Establishments Act in all states. This legislation must ensure that the Charter of Patient’s Rights is observed, it must provide a grievance redressal mechanism to patients, the rates for services must be regulated and standard treatment guidelines should be adopted in healthcare institutions.
Eight, essential medicines and medical devices must be subject to price regulation, based on their manufacturing cost. A Uniform Code for Pharmaceutical Marketing Practices should be put in place to curb unethical marketing practices. Manufacturers should be asked, in a stepwise manner, to sell medicines only under their generic name, and doctors should be directed to write generic names of medicines in prescriptions.
What else is required?
These initiatives must be accompanied by measures to ensure that people with special needs — women, children, differently-abled persons, people living with HIV — enjoy appropriate health services. Traditional social determinants of health such as nutrition, water supply, sanitation and healthy environment must be ensured. There should be plans in place to tackle new determinants like air and water pollution and addictions.
Such a paradigm shift towards a rights-based system for universal healthcare, based on massive increase in health budgets and strengthened health systems, is not an unrealistic dream. Several low- and middle-income countries such as Thailand, Brazil and Sri Lanka have such systems in place. The core ingredient required for UHC is political will. As we prepare to exercise our choice in the elections, we need to boost such political will by supporting parties which have pledged the right to health care to all.
Voting right for undertrials
Why in news?
The Supreme Court is hearing a plea filed by a law student questioning an electoral law which denies undertrials and convicts their right to vote.
What does the law say?
Section 62(5) of the Representation of People Act of 1951 mandates that “no person shall vote at any election if he is confined in a prison, whether under a sentence of imprisonment or transportation or otherwise, or is in the lawful custody of the police”. The provisions however exempt a person held under preventive detention from this rigour.
Intervention in domestic affairs of a country by other country or countries
Why in news?
The revolt against Qaddafi began in Benghazi, and western intervention was legitimised by the fig leaf of a UN Security Council resolution calling for a ceasefire, a no-fly zone and protection of civilians, on which there were five abstentions which included India, Russia and China. Qaddafi accepted the resolution. Shortly thereafter, France, the U.K. and the U.S. attacked Qaddafi’s forces and NATO assumed responsibility for regime change at the same moment that an African Union mediation mission was en route to Libya.
The Libyan tragedy, like those in Iraq, Syria and Yemen, and most probably to ensue in Afghanistan, illustrates wider issues at play.
What’s the broader picture?
Post-Cold-War phenomenon in 1965 and 1981, the UN adopted declarations on the inadmissibility of intervention in the domestic affairs of states, and until the 1990s the UN was the custodian of state sovereignty. The Iraqi Libyan species of intervention, professedly with UN approval but actually under western control, is a post ColdWar phenomenon, the motivation being to implant liberal democratic institutions and human rights, along with security concerns, usually thinly justified by 9/11 and lately the Islamic State. Exogenous state building and a peripheral role for local leaders characterise this innovation in international relations. The spectre of failed states became a major concern, leading to the imposition of a neoliberal agenda in the guise of human rights protection. The ambiguous legal justification for interventions not specifically authorised by the UN, such as the creation of safe havens in Iraq, established a pattern despite negative precedents that showed that attempting nation building in societies divided by ethnic, factional, ideological and religious lines is beyond the capacity of any minority group of UN members, let alone of one superpower. None of the interventions could have taken place without the projection of U.S. power or its indirect underwriting.
Western nations came to contemplate, albeit fitfully and inconsistently, neutralising a number of sovereign states in the third world that were illiberal, war torn or internally weak, as potential threats to international peace. But this essentially political project was presented as a high minded enterprise with altruistic motivations, similar to the post war occupations of Germany and Japan.